Achalasia
Pathology
Achalasia can be either primary (idiopathic) or secondary (e.g. due to Chagas disease). Primary achalasia occurs because of a loss of the myenteric plexus (aka Auerbach plexus) resulting in a lower esophageal sphincter (LES) that can not relax. The LES is hyeprtonic, has a high opening pressure and there is also uncoordinated peristalsis.
Achalasia is associated with an increased risk for esophageal squamous cell carcinoma.
Presentation
Chronic progressive dysphagia to both solids and liquids accompanied by heartburn and bland regurgitation which often leads to weight loss.
Diagnosis
Barium swallow (esophogram): classic “bird-beak” narrowing of the esophagus at the gastroesophageal junction.

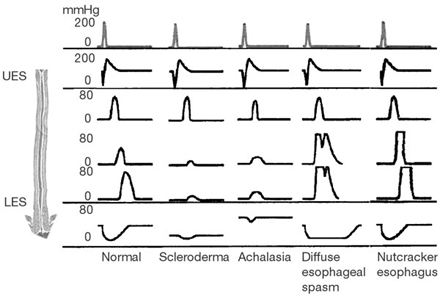
Manometry: hypertonic LES (elevated resting pressure with incomplete relaxation), and reduced peristalsis of the distal esophagus
Management
The current main therapy for achalasia is surgical myotomy. For patients who are not good surgical candidates, pneumatic dilation may be done. If neither of these is an option, there are medications that may help lower the LES pressure.
Resources & Attributions
- Image of barium swallow from the following article: Idiopathic (primary) achalasia. Orphanet Journal of Rare Diseases, Published September 26, 2007; 2: 38. Article and images © 2007 Farrokhi and Vaezi; licensee BioMed Central Ltd. Under CC2.0 licence.

