Renal Cysts and Renal Cancer
Topics: Simple Cysts, Complex Cysts, Renal Cell Carcinoma, Autosomal recessive polycystic kidney disease (ARPCKD), Autosomal Dominant polycystic kidney disease (ADPCKD).
Simple Cysts
Presentation: Small cyst found on asymptomatic screen i.e. incidental cyst. No loculations or septations.
Diagnosis: no further testing required
Treatment: no treatment required
Complex Cysts
Presentation: Can also be found on asymtomatic screen, and will have septations and loculations. However, may present similar to a kidney stone (flank pain and hematuria) or similar to renal cell carcinoma (flank mass, flank pain, hematuria), or with pyelonephritis (when cyst becomes infected).
Diagnosis: Because of the way it presents, a urinalysis and CT scan will usually be done. If pregnant or can’t get a CT scan then an ultrasound. Then this is followed by a biopsy.
Treatment: Disease specific treatment, resection.
Renal Cell Carcinoma
Presentation: Patient with classic triad of flank mass, flank pain, and hematuria. Note that this is only found in about 30% of patients. May also present with paraneoplastic syndromes – the cancer can require a lot of blood causing low hemoglobin, or it can produce erythropoietin (EPO) raising the hemoglobin level (polycythemia). It can also spread hematogenously resulting in a piece of tumor or a DVT in the renal vein or inferior vena cava.
Diagnosis: CT scan or if pregnant an ultrasound. No biopsy because theoretical risk of seeding the peritoneum. The resection done during treatment is acts like a biopsy.
Treatment: Resection – partial or complete nephrectomy.
Autosomal Recessive Polycystic Kidney Disease (ARPCKD)
Presentation: An infant with flank masses, anuria and renal failure on day 1 after birth. Remember this is rare (autosomal recessive).
Diagnosis: Ultrasound then biopsy. Ultrasound shows radially oriented cysts. Because they are so young, not worried about peritoneal seeding. We need the biopsy to ensure it is not renal cancer.
Treatment: supportive care. Transplant could be curative, but likely not to accept a kidney because they are still so young.
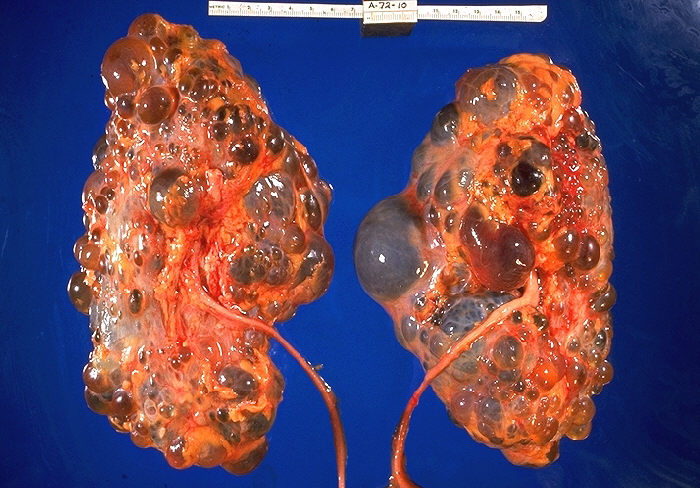
Autosomal Dominant Polycystic Kidney Disease (ADPCKD)
Presentation: Patients start off with little to no cysts but over time the number of cysts increases until they replace most of the renal parenchyma. As a result there is a progression in presentation from an adult who is asymptomatic to one who has hypertension then to someone who has end stage renal disease. Along the way they may present with a flank mass (palpable cysts), pyelonephritis (infected cysts), or hematuria (cysts ruptures and causes bleeding). They can also get complications from developing cysts in other parts of the body: pancreatitis (cysts in pancreas), hepatitis (cysts in liver), deadly subarachnoid hemorrhage (cysts in brain – berry aneurysms).
Diagnosis: CT scan or if pregnant an ultrasound. Then a biopsy . They also need screening for berry aneurysms (MRA, CTA or angiogram).
Treatment: Supportive – treat the hypertension and proteinuria (ACEIs, ARBs) and any other complications. They will at some point require dialysis and they can get a transplant.
Relevant Images



You May Also Like